
New Developments in the Treatment and Management of Heart Failure: Managed Care Considerations on the Evolving Paradigm in HFrEF and HFpEF (JMCM_26.2_Apr2023_web.pdf (jmcmpub.org))
by Alanna A. Morris, MD, MSc
Summary
The management of heart failure has undergone significant changes over the past few years. A four-pillar medication strategy is now recommended and this strategy includes two newer classes of medications which have been shown to improve morbidity, mortality, and hospitalization rates.
Key Points
- ARNI + beta-blocker + MRA + SGLT2i is the new standard of care for heart failure with reduced ejection fraction (HFrEF).
- There are demonstrated benefits of (ARNI) and (SGLT2i) across the spectrum of EF below normal, which includes a subset of those with preserved ejection fraction (HFpEF).
- Morbidity, mortality, and hospitalizations can be reduced with a multidisciplinary and comprehensive disease management program
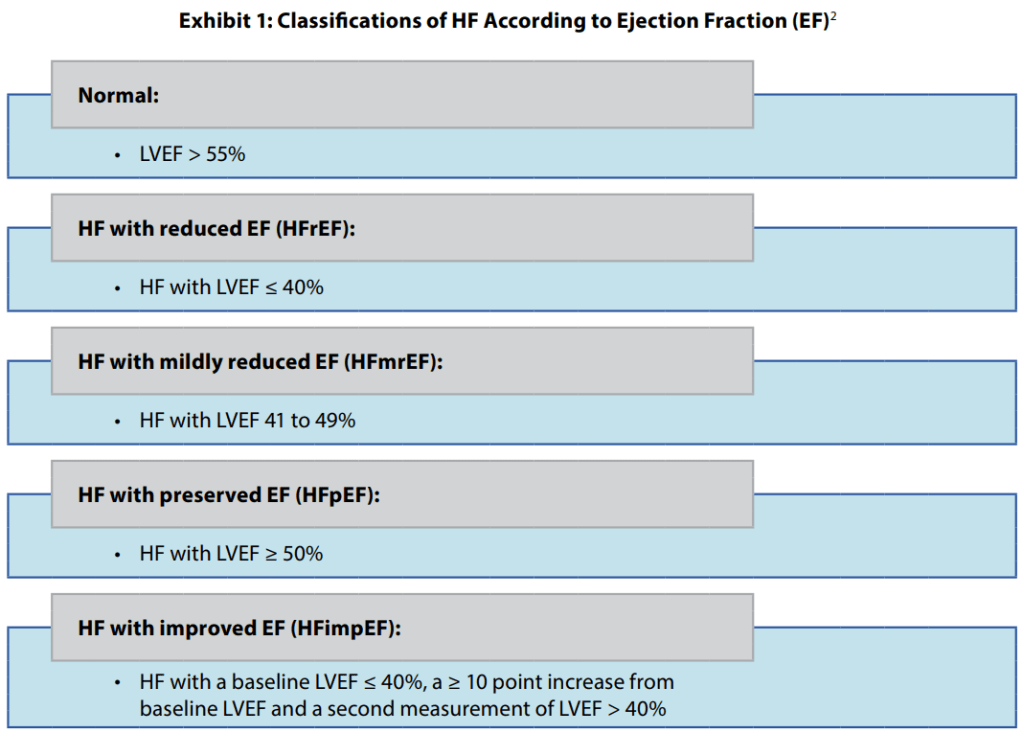
HF is a clinical syndrome with symptoms and/or signs caused by a structural and/or functional cardiac abnormality and corroborated by elevated natriuretic peptide levels and/or objective evidence of pulmonary or systemic congestion.2 HF is classified by ejection fraction (EF)
- The four main pillars of guideline-directed medical therapy (GDMT) for managing heart failure with reduced ejection fraction (HFrEF) include:
- Angiotensin converting enzyme inhibitor (ACE-I) or angiotensin receptor blocker/neprilysin inhibitor (ARNI) combination
- Beta blocker
- Mineralocorticoid receptor antagonist (MRA)
- Sodium-glucose cotransporter 2 inhibitor (SGLT2i)
- Sacubitril/valsartan is the only available ARNI, available only as a brand name product.
- These agents are proven to modify the pathophysiology of heart failure (HF), reducing morbidity and mortality.
- A diuretic may be added for selected patients with volume overload to reduce HF hospitalization and mortality.
- Other agents like isosorbide dinitrate or ivabradine may be added for specific indications.
- Guidelines provide specifics on initiating therapy, starting and target doses, and adherence management. Patients typically start with one agent and add others over time.
- ARNI use is indicated for HFrEF (EF < 40%), NYHA class II–III HF, alongside a GDMT background to reduce morbidity and mortality.
- ACE-I is beneficial for patients with chronic HFrEF symptoms when ARNI use is not feasible, reducing morbidity and mortality.
- ARB is recommended for patients intolerant to ACE-I due to cough or angioedema, and when ARNI use is not feasible, to reduce morbidity and mortality.
- In patients tolerating an ACE-I or ARB with chronic symptomatic HFrEF NYHA class II or III, replacing with ARNI is recommended to further reduce morbidity and mortality.
- SGLT2i, originally approved for type 2 diabetes, now also FDA-approved for reducing CVD morbidity, mortality, and HF hospitalizations due to their benefits demonstrated in randomized control trials.
- SGLT2i therapy is recommended for patients with symptomatic chronic HFrEF to reduce hospitalization for HF and cardiovascular mortality, regardless of type 2 diabetes presence.
- ARNI and SGLT2i have been evaluated across the spectrum of EF below normal, showing benefits in selected patients with HFpEF in decreasing hospitalizations and cardiovascular mortality.
